


BD1 is a complex and chronic mental health disorder characterized by fluctuations between manic and depressive episodes that can cause significant functional impairment and can result in hospitalization.1 BD1 is typically diagnosed in late adolescence or early adulthood after at least 5 years of symptoms, which can vary greatly among individuals, and is often accompanied by other psychiatric comorbidities, including anxiety and substance use disorders.1-3 The lifetime relapse rate of BD1 is up to 90%, with depressive or manic episodes often reoccurring within 2 years of the initial episode.4,5
Following treatment of acute mania, the goal is to prevent its relapse. Antipsychotics can be used as monotherapy or in combination with lithium or an anticonvulsant for the treatment of mania.1,6 Nonadherence to prescribed treatment is a predictor of relapse, but adherence can be difficult to assess in patients.7 LAI formulations of antipsychotics were designed to provide consistent blood concentrations over an extended period of time.2 Missed scheduled injections are also known to providers.7
UZEDY® (risperidone) is FDA-approved as monotherapy or adjunctive therapy to lithium or valproate for the maintenance treatment of BD1 in adults.8 The approval of UZEDY in BD1 was supported by model-informed drug development, which is an approach that leverages existing data in computational modeling and simulation methods to streamline the FDA-approval process.8-10 Population pharmacokinetic models were used to compare exposure levels of UZEDY with another risperidone LAI that was administered intramuscularly.10 Further, the established efficacy of IM risperidone LAI in trials of patients with BD1 was assessed using exposure-response modeling to extrapolate therapeutic equivalence of UZEDY.10 Finally, the safety of UZEDY in BD1 was determined using existing data for IM risperidone LAI in BD1.8
UZEDY makes use of an innovative drug delivery platform called SteadyTeqTM, to formulate an LAI antipsychotic that can be administered subcutaneously.11 Pharmacokinetic studies have demonstrated that following a single dose of UZEDY, therapeutic plasma concentrations are achieved within 6 to 24 hours and maintained throughout the dosing interval, without the need for oral supplementation or loading doses.11,12
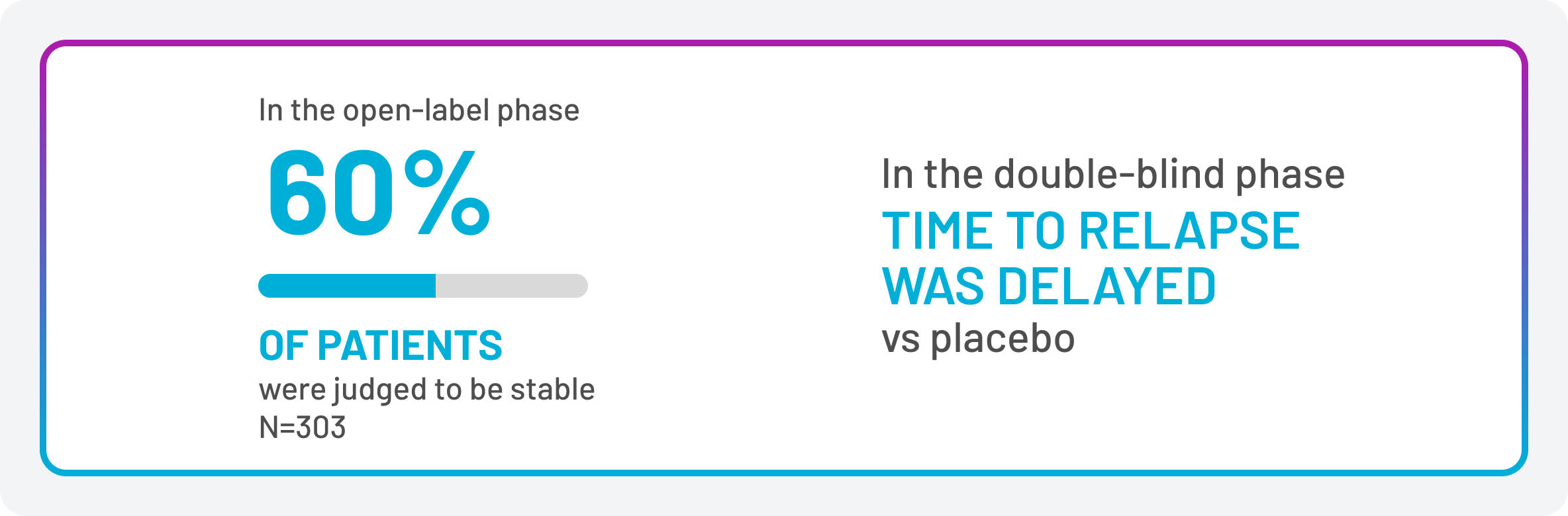
The efficacy of UZEDY as monotherapy for the treatment of BD1 is based on a multicenter, randomized, double-blind, placebo-controlled study of IM risperidone LAI. 501 adults with BD1 initially entered an open-label phase where they received the IM risperidone LAI. After 26 weeks, 303 of the patients (60%) were judged to be stable and were randomized to receive either the same dose of this IM risperidone LAI or placebo. Time to relapse (depression, mania, hypomania, or mixed) was delayed in patients receiving monotherapy with monotherapy IM risperidone LAI (Figure 1).8
Figure 1. UZEDY Monotherapy Provides Delayed Time to Relapse
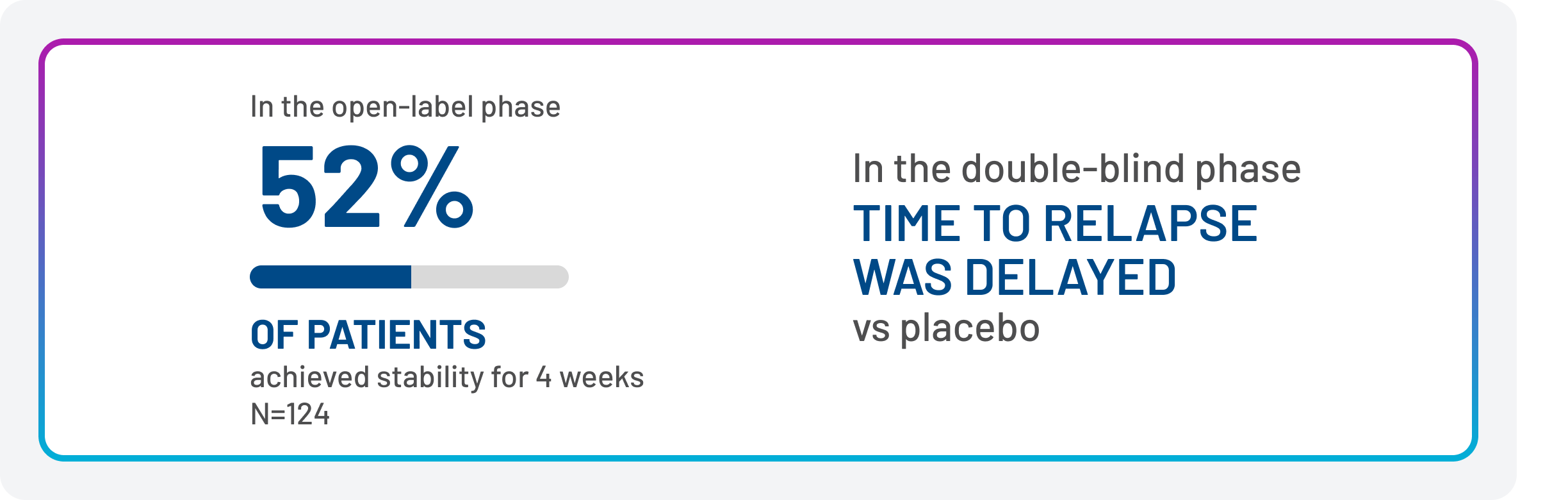
The efficacy of UZEDY as adjunctive treatment of BD1 is based on a multicenter, randomized, double-blind, placebo-controlled study of another risperidone LAI. 240 adults with BD1 were initially treated during an open-label period with the IM risperidone LAI as adjunctive therapy in addition to continuing their usual treatment for BD1.* After 16 weeks, 124 patients (52%) were judged to be stable and were randomized to double-blind treatment with either the same dose of the IM risperidone LAI or placebo, in addition to continuing their usual treatment. Time to relapse (depression, mania, hypomania, or mixed) was delayed in patients receiving adjunctive therapy with the IM risperidone LAI compared with placebo (Figure 2).8
Figure 2. Adjunctive Therapy With UZEDY Provides Delayed Time to Relapse
The safety profile of UZEDY as monotherapy for the maintenance treatment of BD1 in adults is based on adequate and well-controlled studies of the IM risperidone LAI. The safety of UZEDY is expected to be similar to that of the IM risperidone LAI.8
Figure 3 shows the most common adverse reactions reported with the IM risperidone LAI administered as monotherapy in a 24-month double-blind, placebo-controlled trial. Of the patients receiving the IM risperidone LAI, 0.6% discontinued due to an adverse reaction (hyperglycemia; n=1).8
Figure 3. Adverse Reactions Occurring in ≥2% of Patients With BD1 Receiving IM Risperidone LAI as Monotherapy
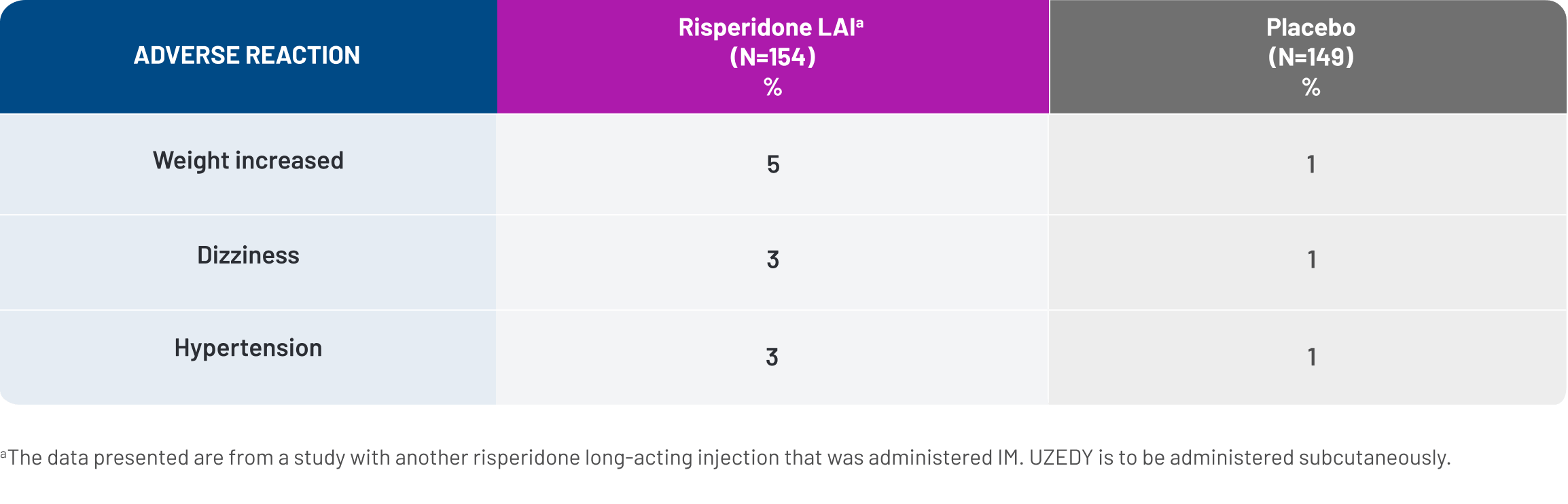
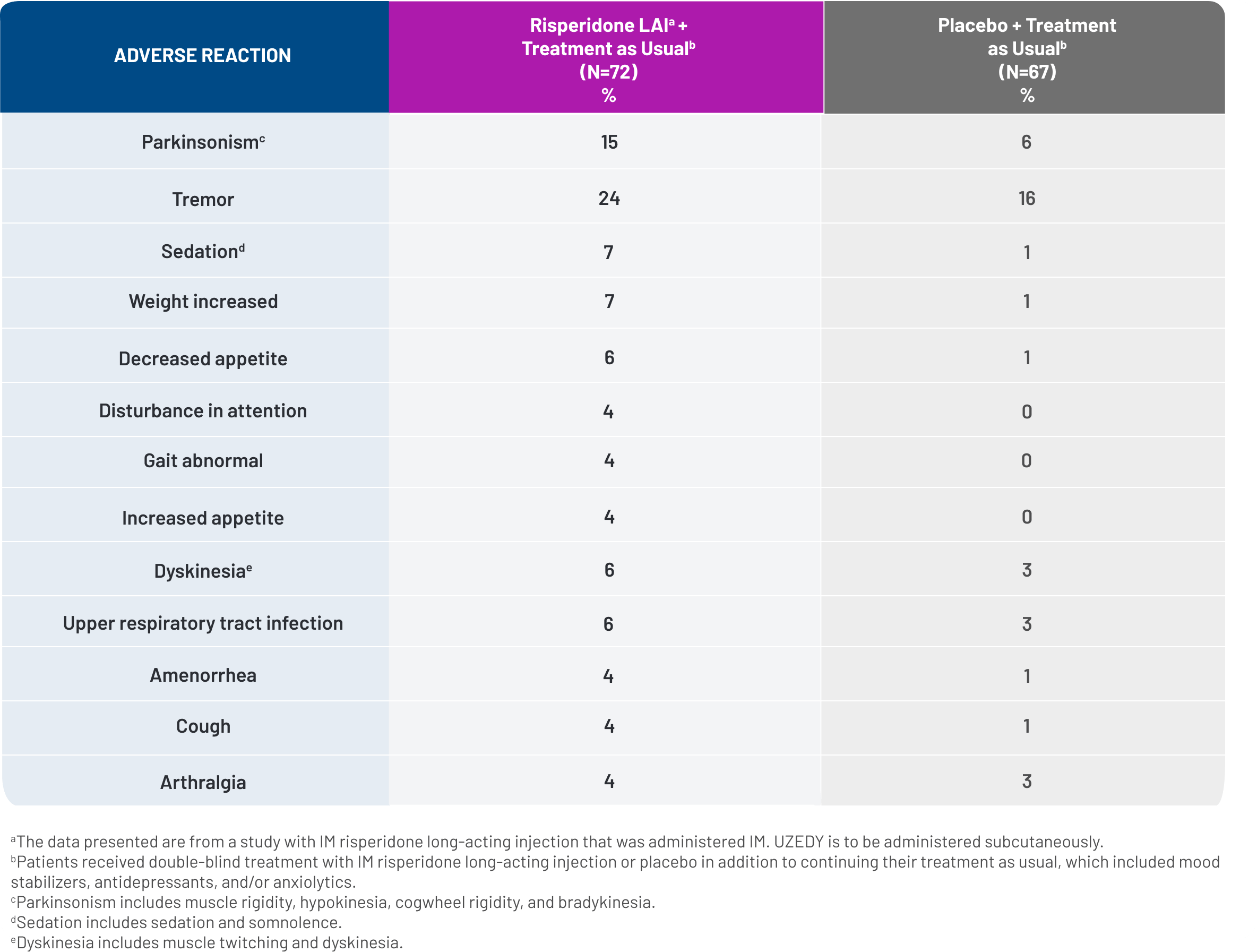
Figure 4 shows adverse reactions reported with the IM risperidone LAI administered as adjunctive therapy in a 52-week double-blind, placebo-controlled trial. Four percent of patients discontinued due to adverse reactions, compared with 1.5% of placebo-treated patients. Adverse reactions associated with discontinuation were hypokinesia (n=1) and tardive dyskinesia (n=1).8
Figure 4. Adverse Reactions Occurring in ≥4% Patients With BD1 Receiving Adjunctive Therapy With IM Risperidone LAI
UZEDY can be started or restarted with a single injection. No loading dose or oral supplementation is required, resulting in streamlined initiation or reinitiation for patients who have missed their regularly scheduled dose.8,11 UZEDY is ready-to-use and comes in a single-dose prefilled syringe with a 5/8-inch, 21-gauge needle for subcutaneous injection in the abdomen or upper arm by a healthcare professional.11
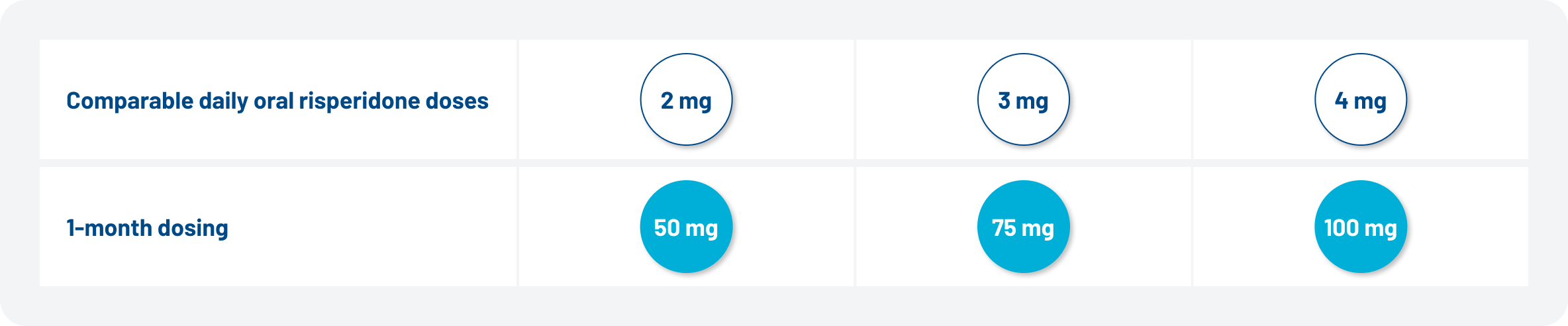
UZEDY is available in 1-month dosing from initiation, with 3 dosage strengths, corresponding to 2 mg to 4 mg oral risperidone, allowing for treatment to be tailored to the individual needs of patients (Figure 5).11 Patients are not required to be stabilized on oral risperidone prior to initiating UZEDY, but tolerability should be established for patients who have never taken risperidone.8
Figure 5. UZEDY Dosing Interval and Dosing Strength Can Be Tailored to the Patient with BD1
- Nonadherence to treatment is a predictor for relapse, which negatively impacts clinical outcomes for patients with BD17,13-15
- LAIs provide consistent dosing within a given timeframe, and providers are aware of a missed scheduled injection2,7
- With UZEDY, therapeutic plasma levels of risperidone are sustained throughout the dosing interval11,12
- UZEDY may delay time to relapse in patients with BD1. Time to relapse was delayed in patients receiving the IM risperidone LAI used as monotherapy or adjunctive therapy8
- The safety of risperidone LAIs has been well established in BD1, and the safety profile of UZEDY is expected to be similar8
- The most common adverse events reported in trials of the IM risperidone LAI were increased weight (5% in a monotherapy trial) and tremor and Parkinsonism (≥10% in an adjunctive therapy trial)8
| * | Treatments consisted of mood stabilizers (primarily lithium and valproate), antidepressants, and/or anxiolytics. All oral antipsychotics were discontinued after the first 3 weeks after the initial injection of IM risperidone LAI.8 |
- Carvalho AF, Firth J, Vieta E. Bipolar disorder. N Engl J Med. 2020;383(1):58-66.
- Vieta E, Tohen M, McIntosh D, Kessing LV, Sajatovic M, McIntyre RS. Early use of long-acting injectable antipsychotics in bipolar disorder type I: an expert consensus. Bipolar Disord. 2025;27(1):7-16.
- Cha B, Kim JH, Ha TH, Chang JS, Ha K. Polarity of the first episode and time to diagnosis of bipolar I disorder. Psychiatry Investig. 2009;6(2):96-101.
- Perlis RH, Ostacher MJ, Patel JK, et al. Predictors of recurrence in bipolar disorder: primary outcomes from the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am J Psychiatry. 2006;163(2):217-224.
- Tohen M, Zarate CA, Hennen J, et al. The McLean-Harvard First-Episode Mania Study: prediction of recovery and first recurrence. Am J Psychiatry. 2003;160(12):2099-2107.
- Butler M, Urosevic S, Desai P, et al. Treatment for bipolar disorder in adults: a systematic review. Comparative Effectiveness Review No. 208. (Prepared by the Minnesota Evidence-based Practice Center under Contract No. 290-2012-00016-I.) AHRQ Publication No. 18-EHC012-EF. Rockville, MD: Agency for Healthcare Research and Quality; August 2018.
- Jawad I, Watson S, Haddad PM, Talbot PS, McAllister-Williams RH. Medication nonadherence in bipolar disorder: a narrative review. Ther Adv Psychopharmacol. 2018;8(12):349-363.
- UZEDY® (risperidone) extended-release injectable suspension Current Prescribing Information. Parsippany, NJ: Teva Neuroscience, Inc.
- US Food and Drug Administration (FDA). Guidance Document. M15 General Principles for Model-Informed Drug Development. Updated November 6, 2024. Accessed August 28, 2025. https://www.fda.gov/media/184747/download.
- Data on file. Parsippany, NJ: Teva Neuroscience, Inc.
- Kane JM, Harary E, Eshet R, et al. Efficacy and safety of TV-46000, a long-acting, subcutaneous, injectable formulation of risperidone, for schizophrenia: a randomised clinical trial in the USA and Bulgaria. Lancet Psychiatry. 2023;10(12):934-943.
- Wagner AM, Elgart A, Perlstein I, et al. Phase 1 open-label study assessing the pharmacokinetics and safety of TV-46000, a novel long-acting subcutaneous injectable formulation of risperidone. Presented at: European Congress of Neuropathology; October 2-5, 2021; Lisbon, Portugal. Poster P.0463.
- Nasrallah HA. Brain damage from recurrent relapses of bipolar mania: a call for early LAI use. Current Psych. 2023;22(8):9-10,54.
- Jones S, Riste L, Barrowclough C, et al. Reducing relapse and suicide in bipolar disorder: practical clinical approaches to identifying risk, reducing harm and engaging service users in planning and delivery of care – the PARADES (Psychoeducation, Anxiety, Relapse, Advance Directive Evaluation and Suicidality) programme. Programme Grants Appl Res. 2018;6(6).
- Hamilton JE, Passos IC, de Azevedo Cardoso T, et al. Predictors of psychiatric readmission among patients with bipolar disorder at an academic safety-net hospital. Aust N Z J Psychiatry. 2016;50(6):584-593.